I conducted ethnographic research across 6 hospitals, interviewing over 100 stakeholders including patients, family caregivers, nephrologists, nephrology nurses, primary care providers, social workers, and healthcare administrators. The interviews were carried out both on-site, immersing myself in the actual care environments where decisions unfold—and online, allowing access to participants who couldn't attend in person.
Interview Framework
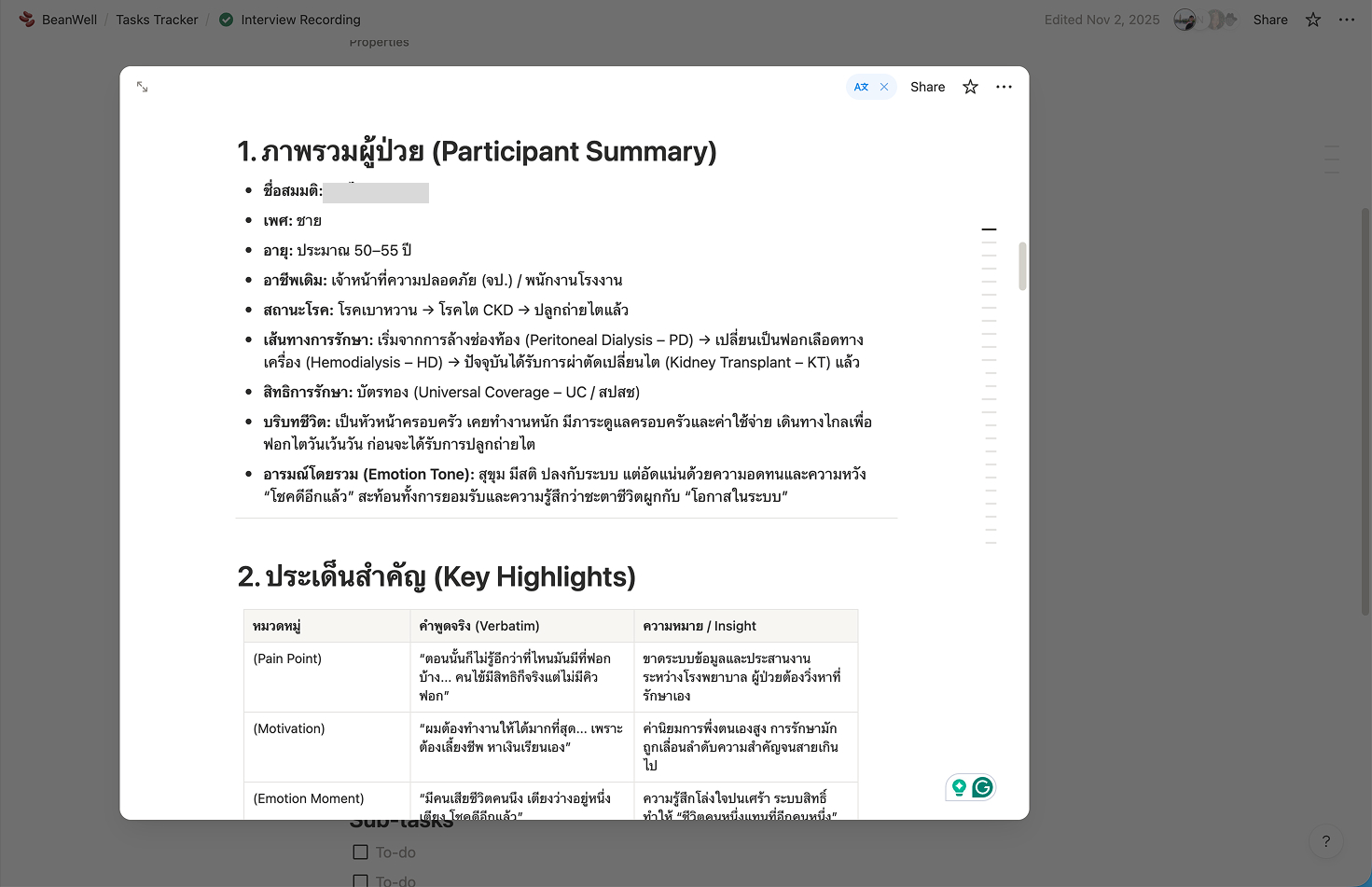
Each interview was carefully recorded and documented in Notion, structured around six key exploration areas:
The patient experience — Understanding the journey from diagnosis through treatment decisions
Relations with other stakeholders — Mapping how different actors interact and influence care
Patient profiles — Capturing demographic, social, and clinical contexts
Cultural probing — Uncovering beliefs, values, and meanings around illness and healing
"What if" questions — Exploring desires and imagined alternatives to current care
Power dynamic questions — Examining the same situation from multiple stakeholder viewpoints
This multi-dimensional framework ensured we captured not just what happens, but why it happens, the beliefs, relationships, and power structures shaping decisions.
Thematic Analysis
The interview transcriptions underwent careful coding and clustering, allowing themes to surface organically from the data rather than imposing predetermined categories. This inductive approach revealed patterns that connected individual stories to systemic dynamics—showing how personal struggles with alternative medicine reflected deeper issues of hope and acceptance within formal healthcare.
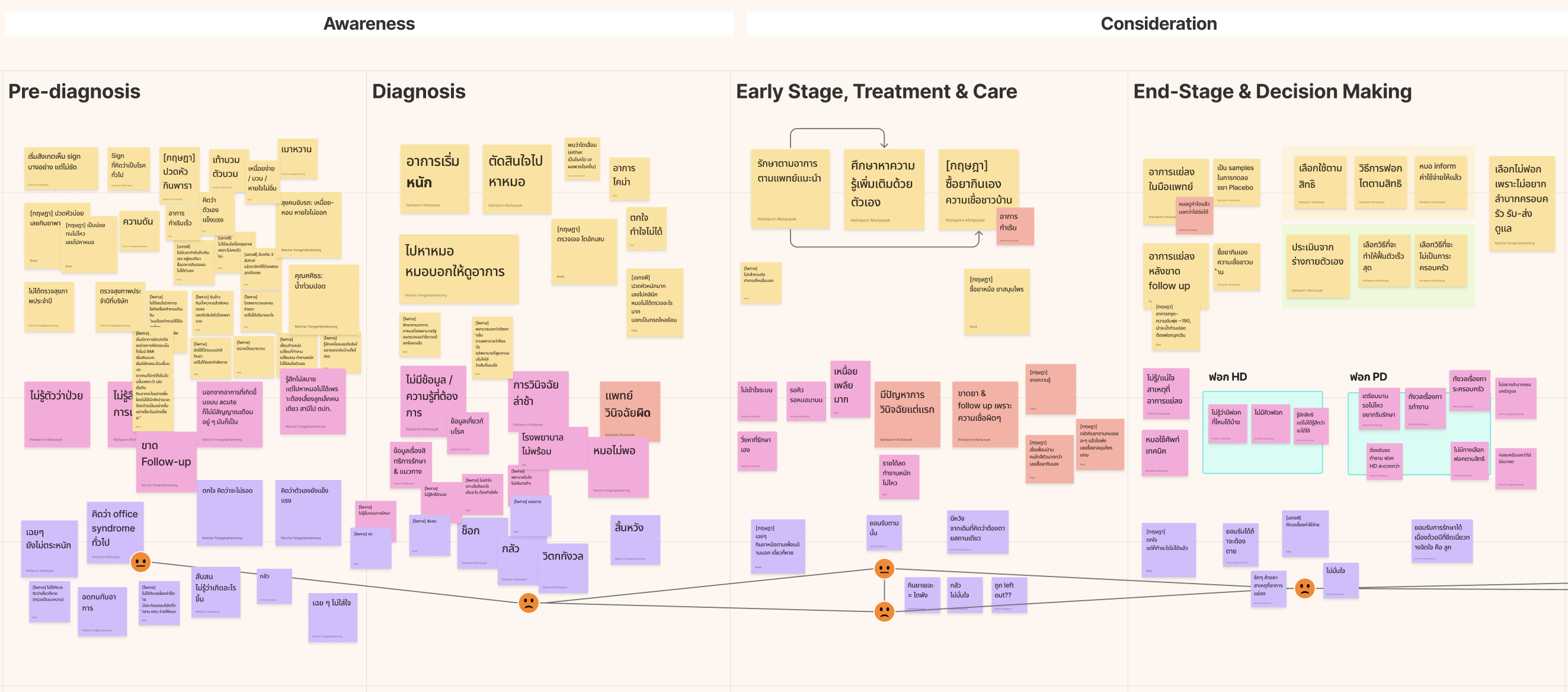
Patient Journey & Service Blueprint
From this research, we consolidated all actions and touchpoints in chronological order, visualising how the disease progresses from pre-diagnosis through to unplanned dialysis. The patient journey map revealed critical gaps, moments where patients fell through cracks, where information failed to reach them, or where cultural beliefs diverged from clinical recommendations.
We also developed parallel journeys for medical service providers; nephrologists, nurses, primary care doctors, to understand how their workflows, constraints, and decision points intersected with patient experiences. This multi-actor service blueprint exposed misalignments: when doctors assumed family understanding, families were still processing shock; when patients needed emotional support, clinicians were focused on clinical protocols.
Ethnographic Film
An ethnographic film is currently in production, translating these insights into a visual narrative that can reach policymakers and practitioners who might not engage with written reports.
Insight Synthesising
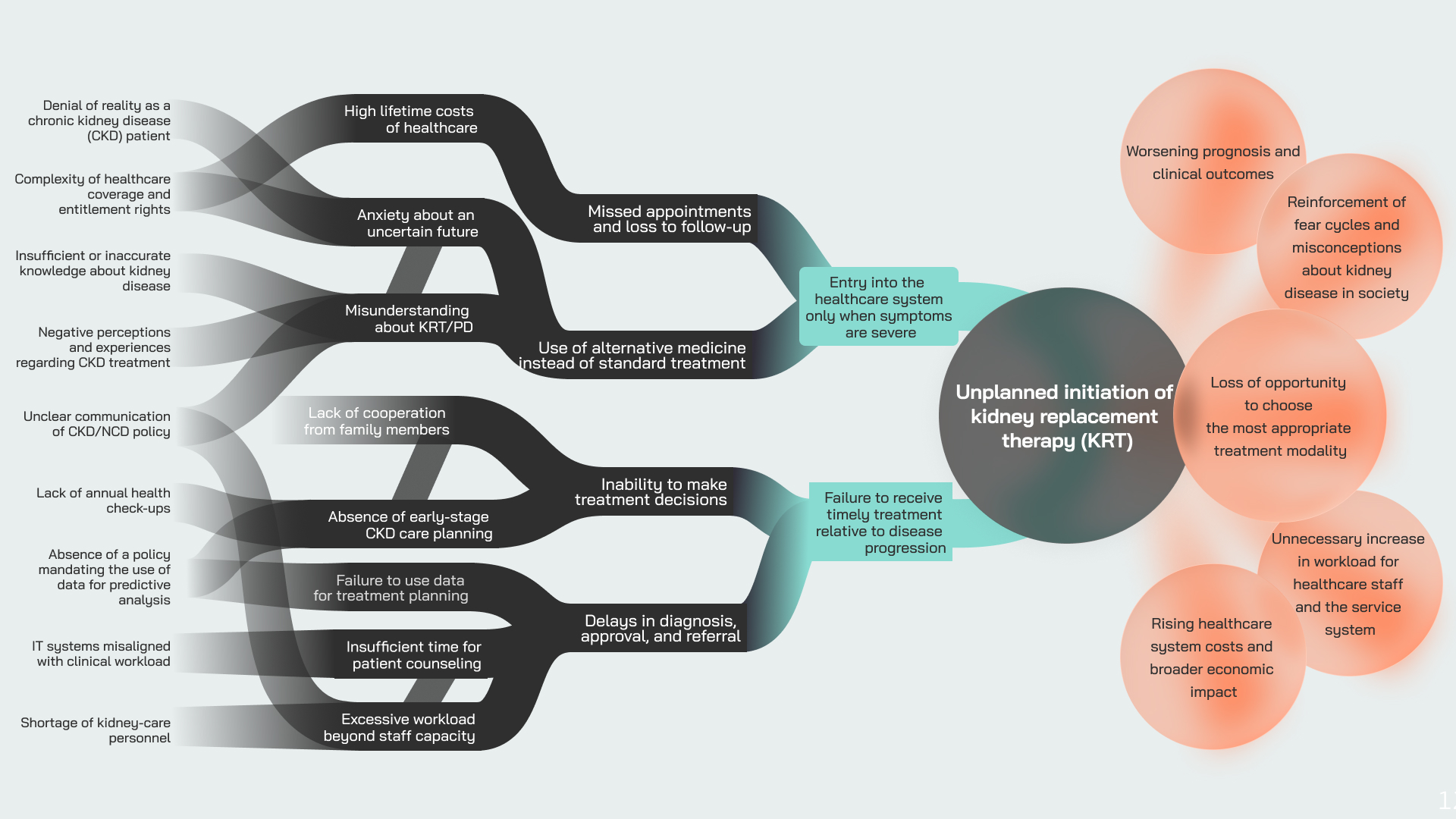
This diagram presents the key themes surfaced from conducting extensive ethnography across 6 hospitals, interviewing over 100 patients, carers, and stakeholders. The synthesis process translated individual stories and experiences into systemic patterns, revealing not just what was happening, but why the system produced unplanned dialysis as a recurring outcome.
Complex systems resist single-perspective analysis. To truly understand how unplanned dialysis emerged as a persistent outcome, we employed multiple mapping formats, each offering a distinct vantage point on the same system, together revealing dynamics that no single tool could capture.
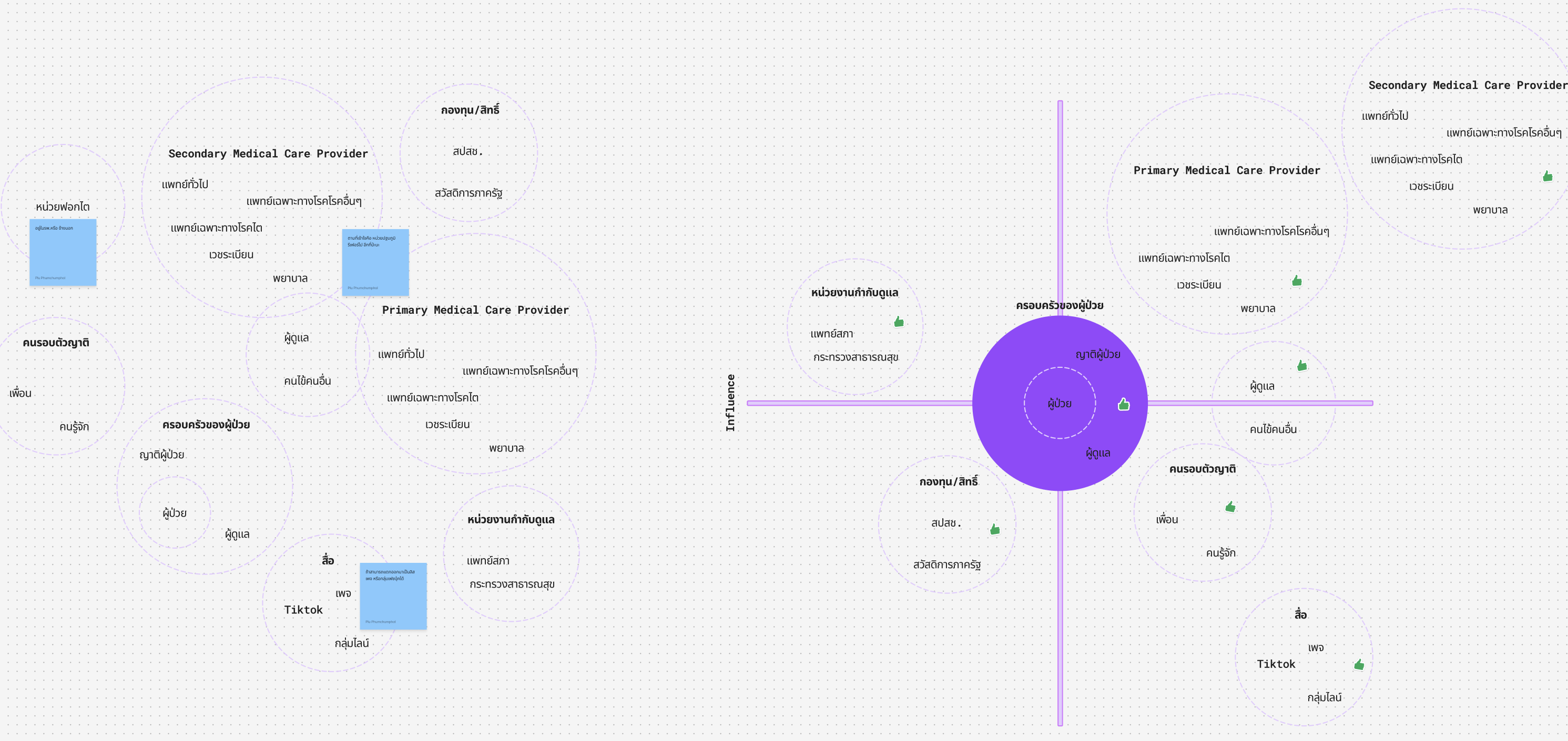
Stakeholder Map: Proximity and Presence
The stakeholder map charted who existed within the CKD care ecosystem and their relative proximity to patients and decision-making. This revealed both visible actors (nephrologists, nurses, patients) and hidden ones (pharmaceutical representatives, traditional healers, community health volunteers), exposing the fuller cast of characters shaping care pathways, often invisibly.
Stakeholder Tension Map: Power and Conflict
Through co-design workshops, we developed a stakeholder tension map that surfaced mutual challenges and power imbalances. This tool made visible the frictions that policy documents obscure: family members pressuring patients based on guilt rather than medical understanding; nephrologists constrained by reimbursement structures that incentivise treatment over prevention; patients navigating conflicting advice from doctors and traditional healers.
The tension map didn't just identify conflicts, it revealed their underlying causes, showing how systemic structures pit stakeholders against each other even when they share common goals.
Causal Loop Diagram: Feedback and Reinforcement
The causal loop diagram traced how actions create feedback loops that either stabilise or destabilise the system. We identified reinforcing cycles, such as how late diagnosis leads to crisis care, which erodes trust, which further delays engagement, and balancing loops that maintain problematic equilibria. This dynamic view explained why good intentions repeatedly failed: the system was designed to produce these outcomes.
Together, these three lenses transformed our understanding from "who does what" to "how the system perpetuates itself", essential groundwork for designing interventions that could genuinely shift systemic patterns rather than merely treating symptoms.
Participatory design in Thailand typically follows established formats: public hearings and questionnaires circulated among 50+ stakeholders, often conducted at a distance from the lived reality of care delivery. For this project, I wanted something fundamentally different:
"Now I would like to involve real patients and frontline workers; we don't want to design from an ivory tower."
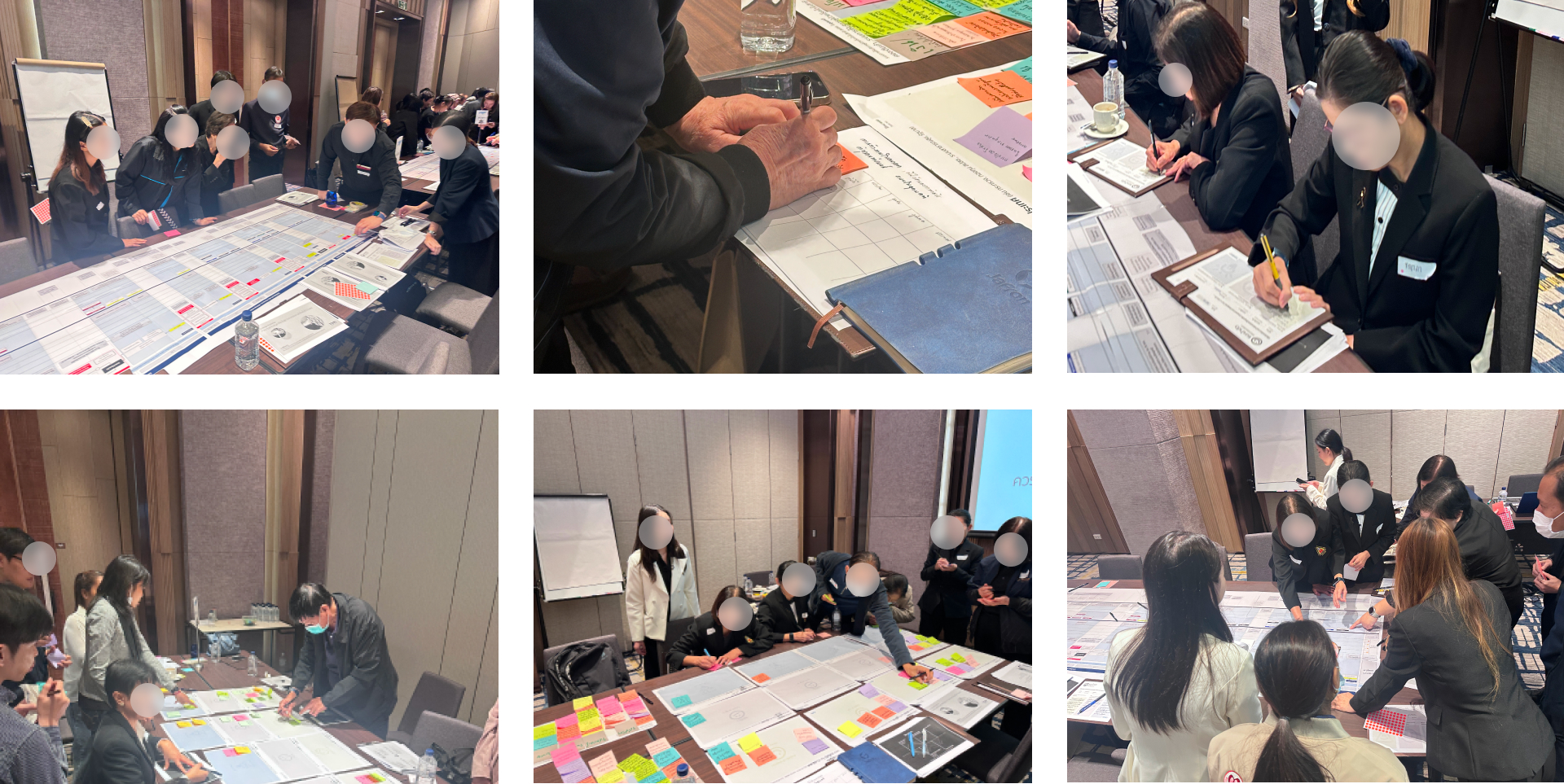
We brought together patients, family caregivers, nephrologists, nephrology nurses, primary care providers, social workers, and policymakers across 6 co-design workshops, each designed to build progressively toward actionable interventions.
Stakeholder Introduction
The first workshop established mutual understanding through designed introduction cards. Rather than standard self-introductions, participants described their power within the system, what blocks them from achieving their goals, and what they're trying to accomplish. This immediately surfaced tensions and dependencies, showing, for instance, how nephrologists feel blocked by hospital capacity whilst patients feel blocked by nephrologists' limited time.
Sense Making Workshop
Using the patient journey map I had created from ethnographic research, we facilitated conversations that bridged experiential divides. Patients shared their stories along the journey; frontline doctors articulated their emotional burdens and systemic frustrations; policymakers revealed constraints they face in changing structures. The journey map became a shared object, allowing each stakeholder to locate themselves and understand how their actions rippled through others' experiences. Empathy emerged not through abstract exercises, but through confronting the concrete reality of how decisions cascade through the system.
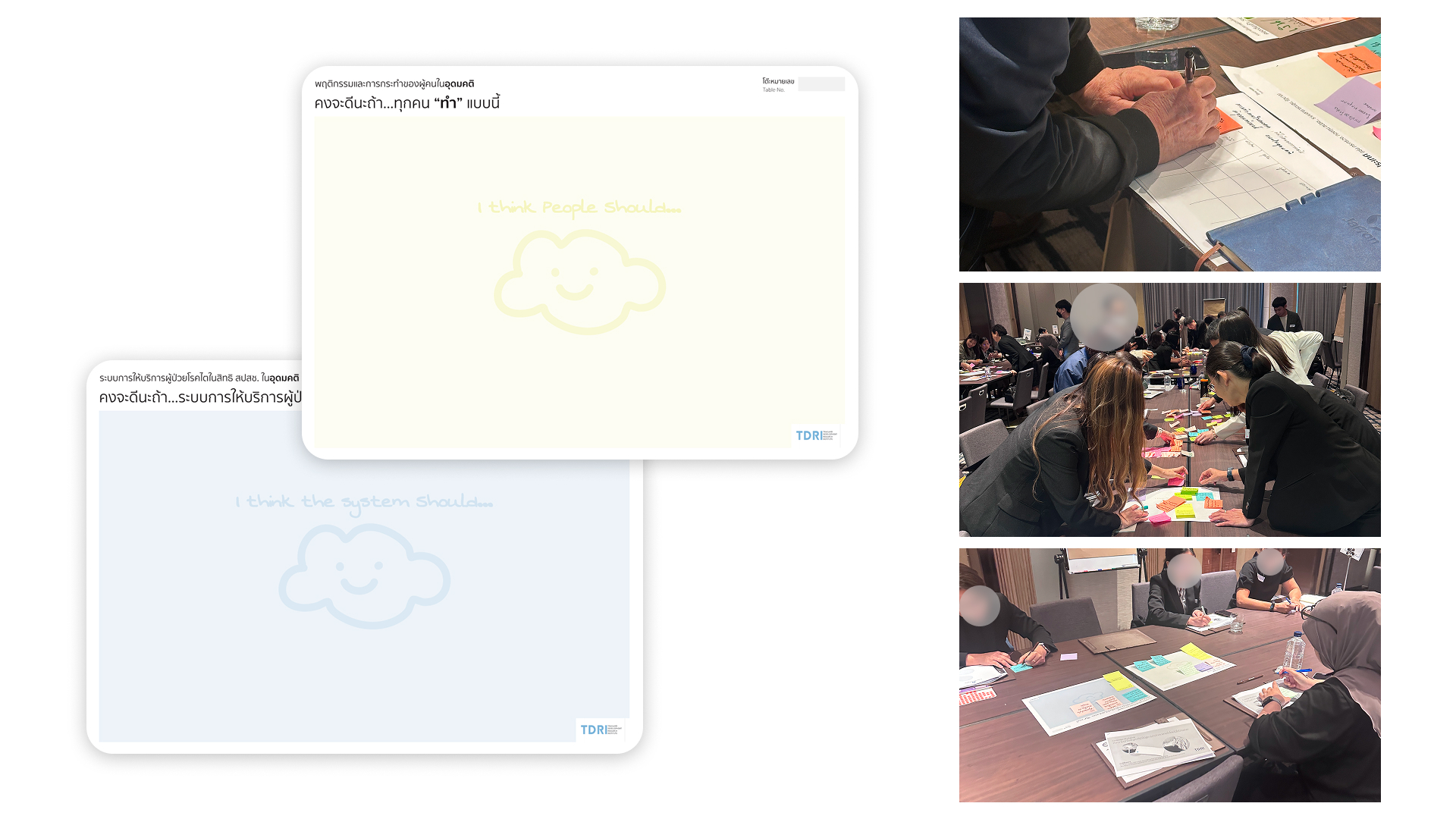
Envision Future
We explored "what if" scenarios and aspirational futures. Rather than asking what's realistic, we asked what's desirable, creating permission to imagine beyond current constraints. Participants articulated futures where patients felt hope within standard care, where families were involved early rather than at crisis moments, where economic barriers didn't determine care access.
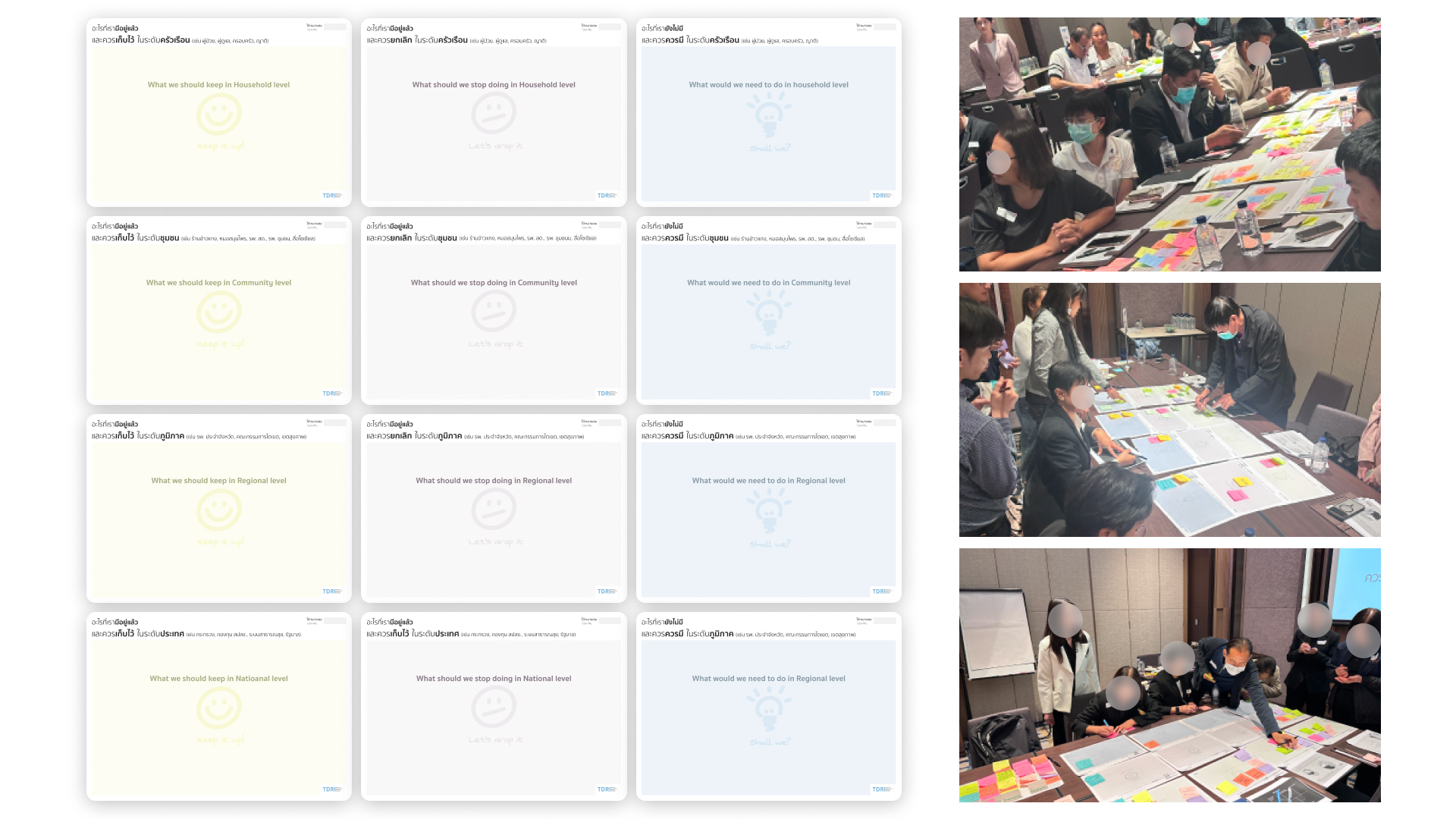
Design Transition
Here we combined solution thinking with the Multi-Level Perspective (MLP), mapping interventions across time horizons. Participants explored what factors we need to keep, discard, and create to move toward envisioned futures, recognising that transformation requires simultaneous shifts at niche, regime, and landscape levels.
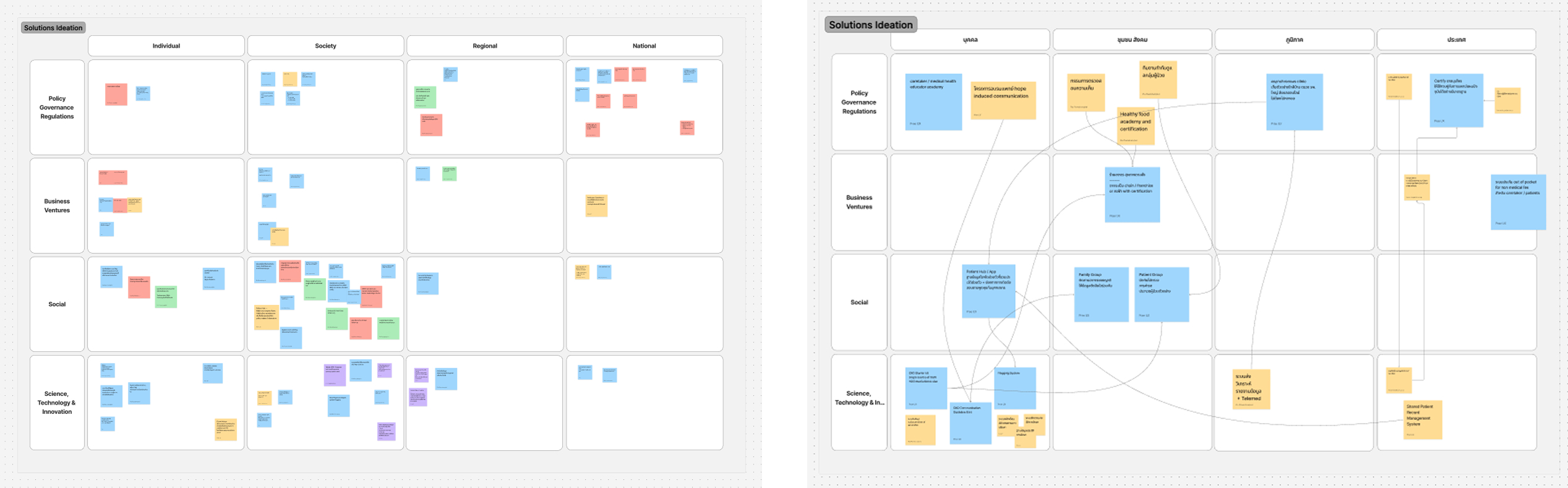
Intervention Ideation
We invited stakeholders to create intervention portfolios through a two-step process: 1. articulate the intervention idea 2. backcast from that idea to identify what prior conditions or interventions must exist to enable it.
This approach prevented "magic bullet" thinking, forcing consideration of dependencies and sequencing. For example, an asynchronous consultation forum requires backend data systems and trained nurses before it can function.
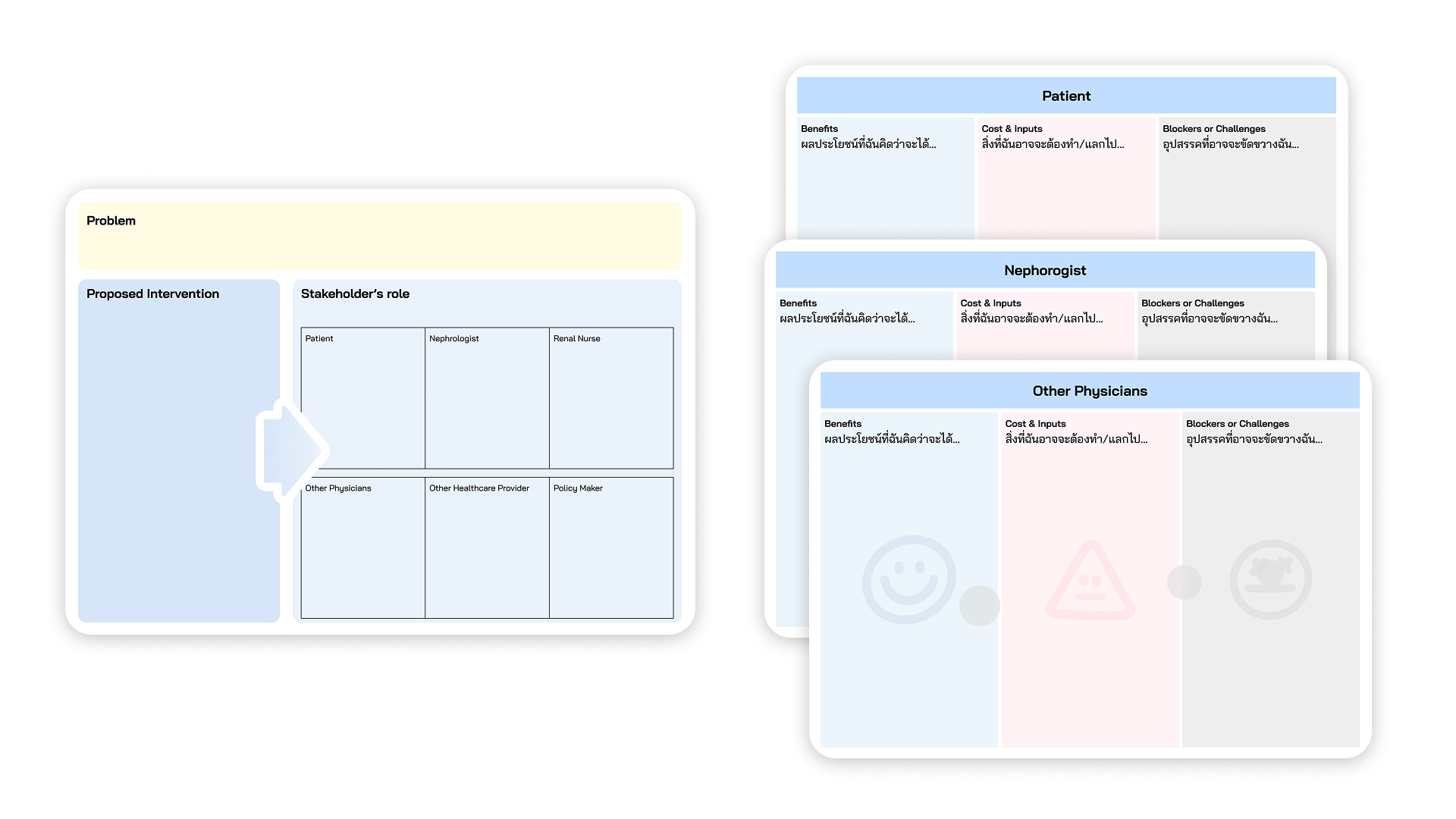
Validating and Putting to Action
Currently underway, this final workshop will validate interventions by exploring risks, consequences, and benefits for each stakeholder group, building buy-in through transparent examination of trade-offs. This process runs alongside the Kano questionnaire, creating both quantitative and qualitative demand articulation that demonstrates not just what stakeholders want, but why certain features matter more than others.
Co-designing ways to prevent unplanned Kidney dialysis for patient under universal health care in Thailand
Year
2025
Role
Lead Service Designer
Design at
Thailand Development Research Institute
Design For
National Health Security Office
5
co-design workshops
80
+ stakeholders involved
8
million people affected
Brief & Challenge
First Transition Design in Thailand
This project represents the first application of Transition Design to reimagine public health services at a national policy level in Thailand. It addresses the urgent challenge of unplanned dialysis among patients with chronic kidney disease (CKD), a persistent problem that requires systemic transformation rather than incremental fixes.
"The project kickstarted from a network of Thai students in the UK who work in policy and were interested in design methods from seeing my work at RCA."
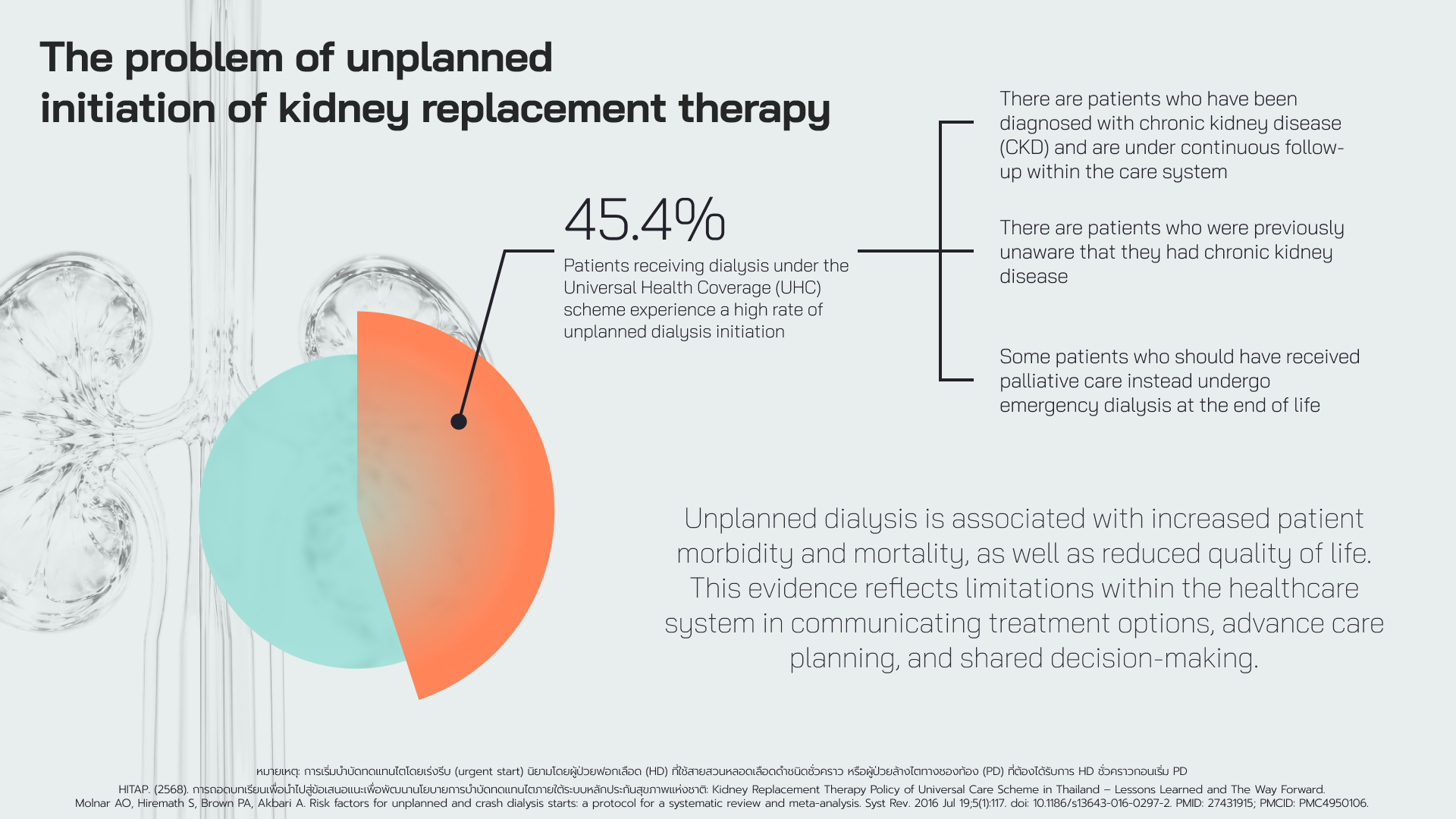
This cross-pollination between design practice and policy expertise created the foundation for what would become a pioneering initiative, bringing Transition Design approaches into Thai healthcare policy for the first time. The project is funded by the National Health Security Office (NHSO), Thailand's primary healthcare financing authority, to tackle the unplanned dialysis crisis. The scale of the problem demanded nothing less than systemic reimagination: Thailand's CKD prevalence stands at 17.6%, nearly double the global average, and unplanned dialysis rates had surged to 60.5% following rapid policy changes in 2022, contributing to approximately 5,500 excess deaths within two years.
Introducing new approach in policy making and public service design
Introducing Transition Design methodology into Thai policy-making presented significant challenges. Thai policy is highly quantitative, favouring established metrics and proven interventions. Gaining approval and buy-in from senior decision-makers, those with the authority to enable or block systemic change, became as crucial as the design work itself.
Building credibility for this new approach required extensive groundwork: comprehensive literature reviews establishing the theoretical foundations, case examples from other countries demonstrating successful systems-level health interventions, and dedicated training sessions to help stakeholders understand and engage with design methods. This preparatory work was essential to bridge the gap between traditional policy-making and design-led transformation.
Design Outcome
Deep dive into Root Causes
We then conducted Causal Loop Diagram (CLD) and Causal Layered Analysis (CLA) synthesis, integrating insights from both ethnographic data and literature review. This multi-method approach allowed us to move beyond surface symptoms to understand the reinforcing dynamics and deeper structures driving the crisis.
The CLD revealed feedback loops, such as how late diagnosis leads to crisis-driven care, which perpetuates patient distrust, which further delays engagement with formal healthcare. The CLA unpacked four layers: the visible problem (unplanned dialysis rates), systemic causes (fragmented care pathways, policy incentives), worldviews (cultural beliefs about medicine and hope), and metaphors shaping how the system understands kidney disease.
Co-Design Workshops: From Sensemaking to Action
We conducted 6 co-design workshops, moving stakeholders through three critical phases: collective sensemaking, ideation, and implementation planning. These sessions didn't just generate ideas, they created legitimate demand articulation for policy change and innovation in public services. When patients, clinicians, and administrators collectively identify needs and co-create solutions, it builds political mandate that traditional top-down policy-making cannot achieve.
We Can't Go Where We Want If We Don't Know Where to Go
From the co-design workshops, I created a future vision by harvesting aspirations from participants and integrating them with the Multi-Level Perspective (MLP) framework from Transition Design. This resulted in a multilevel vision that operates across three horizons, mapping not just the desired future, but crucially, what blocks us from reaching it and what enables us to get there.
The MLP lens allowed us to see how change needs to occur simultaneously at multiple levels: niche innovations (new practices and tools), regime shifts (institutional structures and professional norms), and landscape transformations (cultural beliefs and policy environments). By articulating visions at each level, we could identify specific barriers, from outdated reimbursement structures to deeply held beliefs about hope and medicine, and the corresponding enablers needed to overcome them.
This multilevel vision became a roadmap: showing stakeholders not just an idealised future, but a grounded pathway that acknowledges current constraints whilst identifying concrete leverage points for systemic change.
Exploring Ways to Change
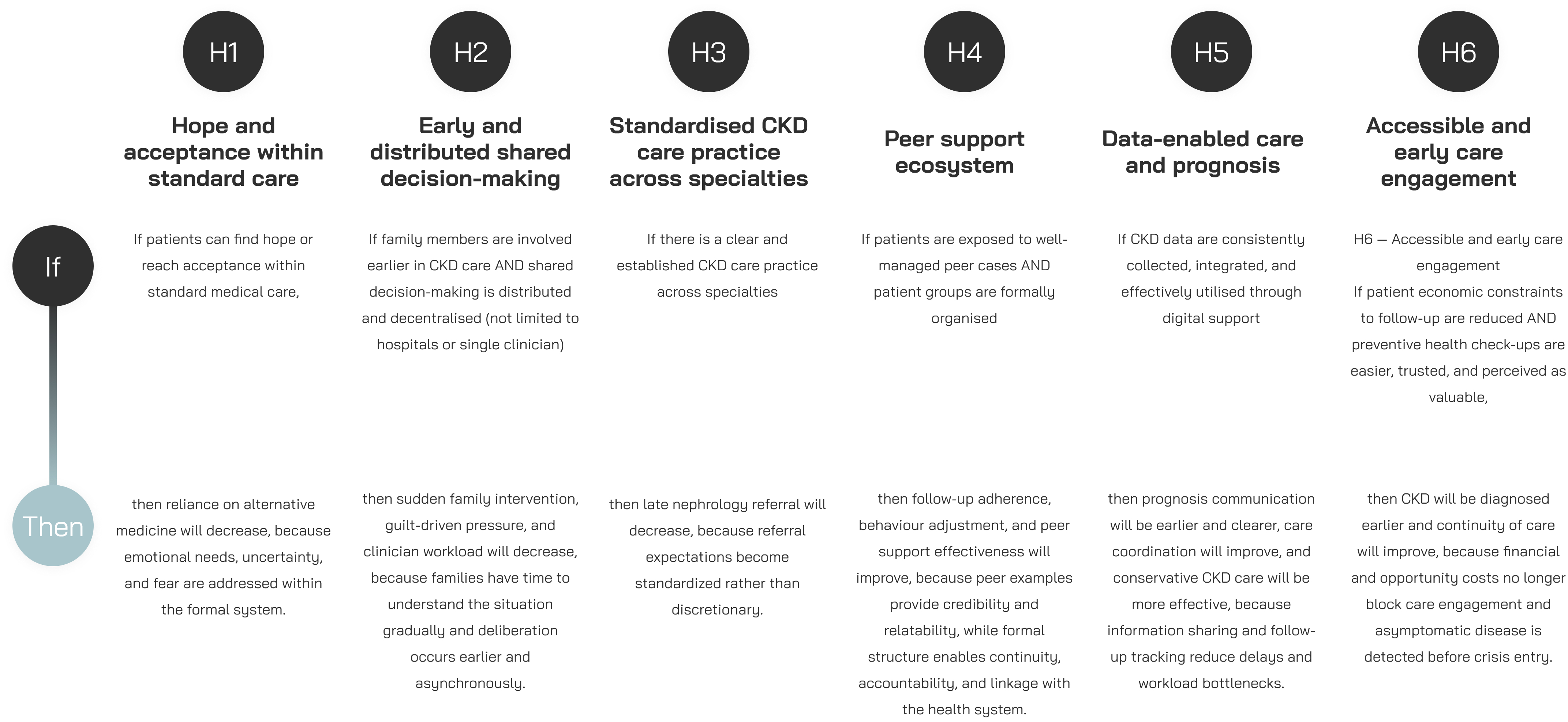
With the multilevel vision established, we needed a rigorous mechanism to translate aspirations into actionable interventions. We employed Theory of Change methodology, beginning with the development of hypothesis stacks, explicit assumptions about how change occurs in complex systems.
Rather than jumping directly to solutions, we first articulated the causal logic: if [condition], then [outcome], because [mechanism]. This approach forced us to make our assumptions testable and transparent. Each hypothesis identified a specific leverage point in the system, from enabling hope within standard care to distributing decision-making across time and space, and specified the change pathway we believed would create impact.
These hypotheses became the foundation for intervention design, ensuring that every solution we developed was grounded in an explicit theory about how the CKD care system could transform. By making our logic visible, we created accountability: these weren't just good ideas, but falsifiable propositions that could be tested, refined, or abandoned based on evidence.
The project is now moving into solution development; co-creating an ecology of interventions designed to work together rather than in isolation.
What's next
The project is now moving into its delivery phase, producing a suite of interconnected outputs designed to translate research and co-design into actionable change:
Portfolio of Solutions
An ecology of 11 interventions designed to work together rather than in isolation; from digital family platforms to peer mentor programmes to prevention accountability systems, each grounded in our hypothesis stack and validated through stakeholder engagement.
Roadmap Through Three Horizons
A strategic implementation pathway mapping solutions across short-term (Horizon 1), transitional (Horizon 2), and transformative (Horizon 3) timeframes, showing dependencies, enabling conditions, and sequencing for systemic change.
Ethnographic Film
A visual narrative translating complex research insights into accessible storytelling, designed to reach policymakers and practitioners who may not engage with written reports, humanising the data and building emotional investment in change.
Policy Blueprint
Detailed guidance on execution mechanisms: what legislative changes are needed, which agencies must coordinate, what funding structures should shift, and how accountability can be embedded, bridging the gap between vision and implementation.
Future State Service Journey
A reimagined patient experience map showing what CKD care looks like when these interventions are in place; from diagnosis through treatment decisions, making the vision concrete and tangible for stakeholders.
Demand Articulation Report
Quantitative and qualitative evidence from the Kano questionnaire and validation workshops demonstrating stakeholder priorities, feature categorisation (must-be, performance, delighters), and the legitimate demand base for proposed changes.
Policy Recommendation Report
Consolidated recommendations for NHSO and Ministry of Public Health, synthesising all project learnings into actionable policy directions with clear rationale, evidence base, and implementation considerations.
Reflection
As we've progressed through this project, several unexpected realisations have emerged, some challenging assumptions I held about co-design in hierarchical cultures, others affirming the power of well-crafted participatory processes.
Breaking Through Cultural Reserve
Perhaps the most surprising discovery has been how genuinely fun and enriching the process has become. Thai culture is typically reserved; people don't readily offer critical commentary or challenge established norms, making co-design workshops notoriously difficult to facilitate.
With carefully designed toolkits and activities, we managed to create spaces where patients spoke up even in the presence of doctors, a profession held in extraordinarily high regard in Thailand.
This wasn't about diminishing professional authority, but rather creating legitimate channels for diverse voices to contribute expertise. Patients became experts in lived experience; families articulated care coordination needs; doctors recognised systemic constraints they couldn't solve alone. The right scaffolding proved that co-design can work exceptionally well in hierarchical cultures, perhaps even more powerfully than in individualistic ones, if the process honours existing social dynamics whilst creating permission structures for authentic dialogue.
Institutional Validation
The project has gained significant institutional endorsement, with opportunities to present to the Board of Kidney Disease. This visibility has drawn considerable attention not just to the CKD care challenge, but to Transition Design methodology itself, demonstrating that rigorous, participatory design approaches can earn credibility within highly technical, policy-driven environments.